


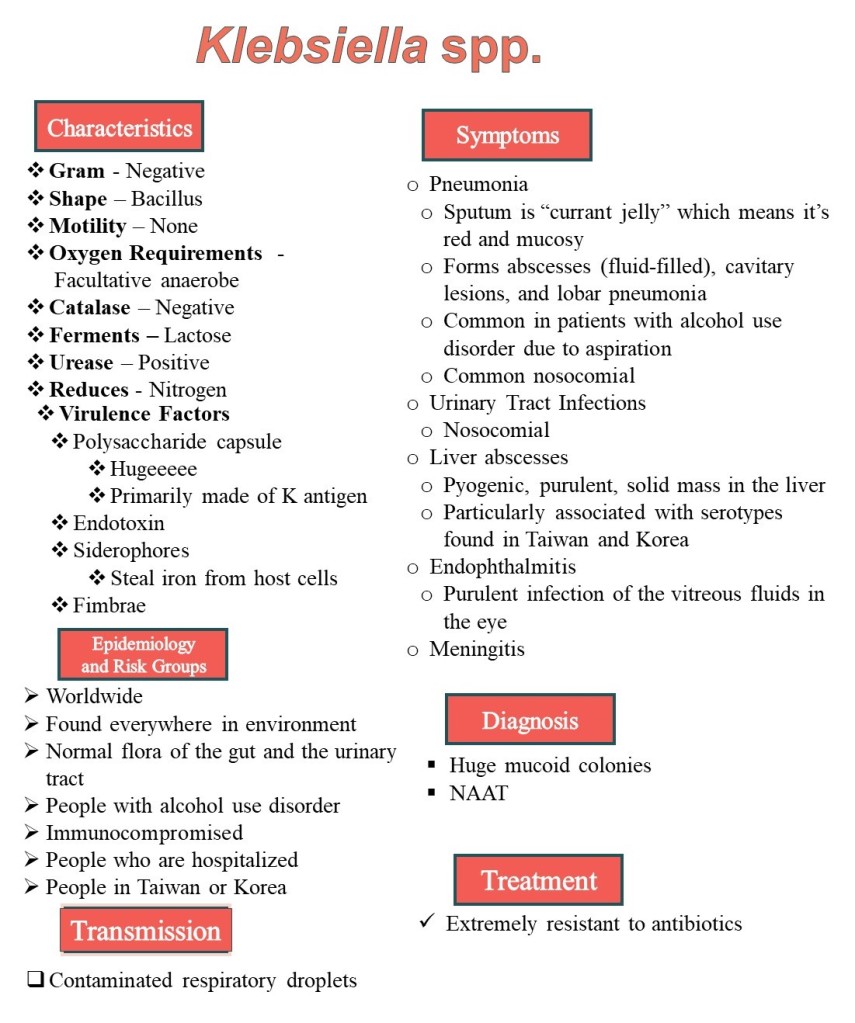
Klebsiella pneumoniae is the most well-known species of the genus Klebsiella. These organisms are often the cause of pneumonia, but can also cause urinary tract infections, liver abscesses, endophthalmitis, and meningitis.
Pneumonia caused by Klebsiella spp. causes a lobar pneumonia that might also form fluid-filled abscesses and cavitary lesions. The sputum is often described as being “currant jelly” which is a very red, jelly-like substance because of a large amount of mucus and blood. People who have alcohol use disorder, are hospitalized, or are immunocompromised might be more susceptible to acquiring this infection. This is typically acquired by aspiration.
Klebsiella spp. can cause the formation of purulent, solid masses in the liver with accompanying fever and abdominal pain. The serotype that causes liver abscesses is particularly associated with Taiwan and Korea.
There are many different serotypes of Klebsiella spp. which are identified by their K antigens which make up the huuuuge polysaccharide capsules. These huge capsules are the primary virulence factor and make it nearly impossible for the immune system to “see” the bacterium. Siderophores are another virulence factor that steals iron from host cells. Klebsiella spp. also has fimbrae which helps the bacterium attach to cells, which is particularly important during urinary tract infections.
Klebsiella spp. are very often found in the hospital, so multi-drug resistance is becoming a really big problem. Nearly all Klebsiella spp. infections should be tested for susceptibility.

A 63-year-old male presents to the hospital with fever, loose stools, and a lack of appetite for 1 week. Vital signs reveal a fever. Past medical history reveals a 25-year history of poorly controlled diabetes mellitus type-II. Physical examination reveals a mild non-tender, hepatomegaly, 2 cm from the right costal margin. Ultrasonography reveals a large, ill-defined hypoechoic lesion in the right lobe of the liver at segments VII and VIII measuring 8x6x5 cm. Laboratory results reveal blood leukocytosis with a neutrophil predominance. Urinanalysis revealed the presence of protein, blood, and WBCs, but no bacteria. Serum creatinine levels were 647 mcgram/L. The lesion in the liver was aspirated and produced a thick pus. Blood cultures reveal an organism that produced pink colonies on Eosin-Methylene Blue agar, and pink colonies on MacConkey agar. What is the capsule of the most likely organism made of?
A. Type-4 pili
B. Kleb proteins
C. Opa proteins
D. K antigens
First, diagnose the patient.
The patient is presenting with systemic symptoms of an infection. He has poorly controlled diabetes mellitus type-2, which suggests that he’s immunocompromised. The urinanalysis findings suggest acute kidney injury is occurring.
The finding of hepatomegaly, and the lesion is suggestive of a liver abscess. Liver abscesses are most commonly caused b Escherichia coli, and Klebsiella pneumoniae.
Pink colonies on MacConkey agar is suggestive of a lactose fermenter. Pink colonies on EMB agar is suggestive of a lactose-fermenter, but the lack of a green, metallic sheen rules out E. coli. Therefore, the patient has a Liver abscess caused by K. pneumoniae.
The capsule of K. pneumoniae is very large and composed mainly of the polysaccharide called “K antigens” the differences between the antigens determines the serotype.
Therefore,

References:
https://microbewiki.kenyon.edu/index.php/Klebsiella_pneumoniae
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6167513/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6435446/
https://jmedicalcasereports.biomedcentral.com/articles/10.1186/s13256-018-1924-4
